Laparoscopic Adjustable Gastric Banding
How it works:
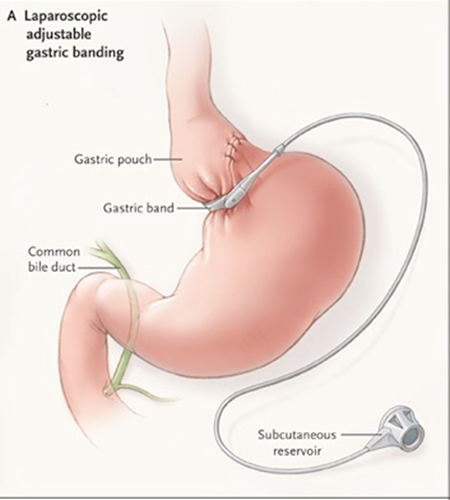
The adjustable gastric band is only a restrictive procedure. The small intestine is not altered during this procedure. Currently two types of gastric bands are on the market in the United States: the “Lap-Band System”® and the newer “Realize Band”™. The adjustable silicone ring is placed around the stomach 1-2 cm centimeters below the esophagus (see figure). This ring is attached to tubing, which is threaded under the skin to a round “port”. One can feel this port just under the skin in the center of the abdomen. This is how the surgeon adds or subtracts water to make the band smaller or bigger.
What to expect afterwards:
After adjustable gastric banding, one must get used to eating solid foods again. The regimen typically starts with two weeks on a liquid-only-diet, two weeks of semi-solid pureed foods and then solids. The stomach needs to heal from surgery before the first fill. So the first adjustment won’t occur until around six weeks after surgery. Gastric bands need to be adjusted an average of four to six times in the first year after surgery. These fills are done to make sure the band is not too tight or too loose and/or to encourage continued weight loss. Band adjustments are painless, and are usually done in the Radiology department under direct vision so the surgeon can see how tight to make the band in order to restrict food intake, but not make it so tight that one can’t eat or drink anything. After surgery the patient must be mindful about what, how and when to eat. This includes eating smaller meals, because the new stomach can hold only about a quarter-cup to a full cup of food at a time. Sometimes people who have undergone gastric banding can eat a lot, and sometimes they can’t eat anything. It is important to “listen to the band” and not just try to eat the same amount each day. It is also important to chew carefully and stop eating when one feels full, or nausea and vomiting can occur. Don’t eat and drink at the same time, because this may increase the chance of discomfort and vomiting.
Even though there is no stomach or intestine cut or stapled the procedure still has risks associated with it
Risks and complications include:
- Bleeding
- Infection
- Slippage of the band can occur with persistent vomiting if behavioral changes are not made.
- The band may erode into the inside of the stomach.
- The band can spontaneously deflate due to leakage.
- The stomach pouch can enlarge.
- The stoma (stomach outlet) can be blocked.
- Gastroesophageal reflux disease or GERD, when stomach contents rise up into the esophagus (the tube that carries food from the mouth to the stomach).
- Death. The risk of death due to gastric banding surgery is about one in 2,000.
- Frequent visits for band adjustments or fills.
- The pouch may stretch with continued overeating.
Compared with other types of weight loss surgery, adjustable gastric banding has these advantages:
- Reversible
- Adjustable
- Less invasive
- Can be done on an outpatient basis
- Does not interfere with absorption, so vitamin deficiencies are less likely to occur.
- Lower risk of dumping syndrome, which occurs when the undigested stomach contents are “dumped” into your small intestine too quickly. It is marked by abdominal cramps and nausea.
- Improves health problems related to excessive weight, including type 2 diabetes, high cholesterol, sleep apnea, high blood pressure and asthma.
- Slow and steady weight loss
Long Term Results:
The expected amount of excess body weight lost from the procedure is about 30-50% at one year. The New England Journal of Medicine article. However these results are based on a very compliant patient population. It is important to remember that this is not a quick fix to loose weight. Long-term success requires a life long commitment to behavior modifications, in eating habits and a regular exercise program. Because we feel strongly that the success of the adjustable gastric banding falls largely on the compliance of the patient we are more selective in the patients that we offer this procedure to.
Relevant Articles Published by Dr. Frantzides on this Procedure
Madan, A, Zografakis J, Frantzides CT; Laparoscopic Adjustable Gastric Banding; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Frantzides, C.T., Welle, S., Laparoscopic Conversion of Adjustable Gastric Band to Roux-en-Y Gastric Bypass .Video Atlas of Advanced Minimally Invasive Surgery. Sounders Elsevier 2013
Frantzides, C.T., Welle, S., Laparoscopic Removal of Eroded Adjustable Gastric Band and Conversion to Roux-en-Y Gastric Bypass with Partial Gastrectomy. Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier 2013
Frantzides C. T., Frantzides A. T., “Laparoscopic Revision of Failed Bariatric Procedures, J. Surg. Sc., in Press, 2018
Want to Know More About Dr. Frantzides? See what others are saying: www.ObesityHelp.com